V6 - Endoscopic Intermuscular Dissection for Large, Obstructing Subepithelial Tumor of the Transverse Colon Using the Novel Dynamic Rigidizing Overtube
Assistant Professor of Medicine Saint Louis University St. Louis, MO
Marina Kim, DO1, Tamadar Abdulrhman Al Doheyan, MD2, Roshan Raza, MD2, Mohamed Othman, MD2 1Saint Louis University, St. Louis, MO; 2Baylor College of Medicine, Houston, TX
Introduction: Colon lipomas, rare benign tumors (<1% incidence in colonoscopies), mainly arise from the submucosa. Larger ones ( >4 cm) pose risks of obstruction, bleeding, and perforation. Surgical excision is standard, but endoscopic techniques are emerging. Conventional methods carry perforation risks due to adipose tissue's poor energy conduction. Novel approaches like "loop-and-let-go" and "unroofing" are explored. We present a case of modified endoscopic submucosal dissection (ESD), termed endoscopic intermuscular dissection (EID), using a dynamic rigidizing overtube for en-bloc resection of a giant transverse colon lipoma.
Case Description/Methods: A 62-year-old man was referred for endoscopic resection of an incidentally found 4cm pedunculated polyp in the transverse colon on routine screening colonoscopy. The patient received general anesthesia with endotracheal intubation and was paralyzed for the procedure. Peak pressures were monitored during the case. A pediatric colonoscope (PCF-H190DL, Olympus America, Center Valley, Pa, USA) with a tapered-tip distal attachment cap (ST hood, Fujifilm Medical Systems, Stamford, Conn, USA) was introduced through a rigidizing overtube. The lesion was identified as having a very thick stalk and the technique began as a standard ESD with a semi-circular mucosal incision. Adequate submucosal lift was achieved with a standard lifting solution. A 2mm needle knife (ORISE ProKnife, Boston Scientific) was used for mucosal incision and submucosal dissection. During the dissection, the lesion was noted to be arising from the muscularis propria and the knife was used to carefully dissect the muscle fibers, taking specific care to not rupture the capsule of the lesion. The defect was first approximated using the hold-and-drag technique of the anchor pronged clip (MANTIS clip, Boston Scientific) followed by complete closure with conventional clips.
Discussion: Total procedure time was 41 minutes. Histopathology revealed a 4cm x 2.5cm intermuscular lipoma, resected en-bloc with clear margins. Same-day discharge followed. Intermuscular lipomas are rare in colonic resections, posing challenges for resection. EID has been performed in the rectum but this is the first report of this procedure in the colon. Colonoscope stability and maneuverability are vital in successfully performing colonic ESD and EID; the novel rigidizing overtube ensured safe resection. Further studies are crucial to refine resection strategies for large colonic lipomas.
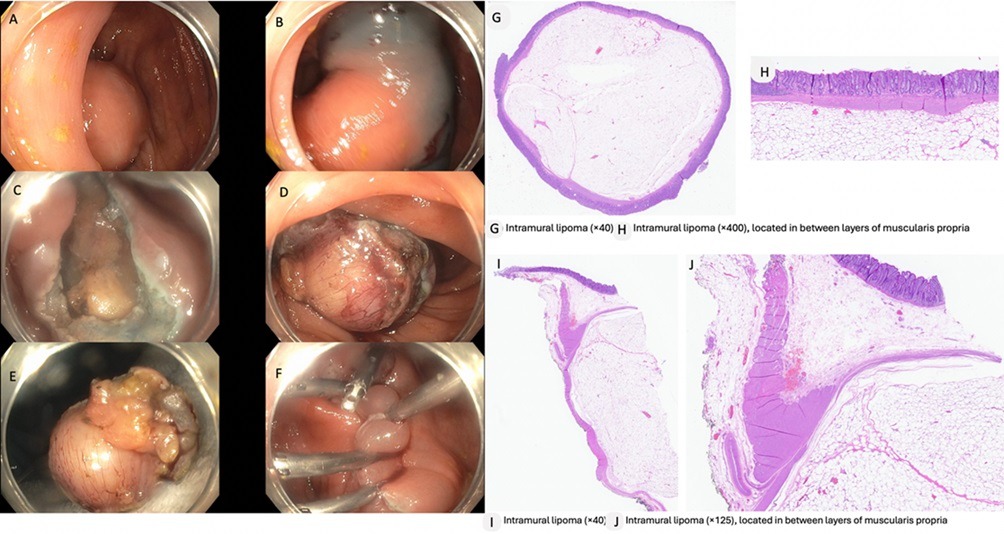
Figure: A,B: Giant lipoma in the transverse colon, C: Post resection defect showing longitudinal muscle fibers of the muscularis propria and submucosa, D,E: Resected lipoma, F: mucosal closure with clips, G: Intramural lipoma x40 mag, F: Intramural lipoma x400 mag, located between layers of muscularis propria, I: Intramural lipoma x40, J: Intramural lipoma x 125 mag, located between layers of muscularis propria
Disclosures:
Marina Kim indicated no relevant financial relationships.
Tamadar Abdulrhman Al Doheyan indicated no relevant financial relationships.
Roshan Raza indicated no relevant financial relationships.
Marina Kim, DO1, Tamadar Abdulrhman Al Doheyan, MD2, Roshan Raza, MD2, Mohamed Othman, MD2, V6, Endoscopic Intermuscular Dissection for Large, Obstructing Subepithelial Tumor of the Transverse Colon Using the Novel Dynamic Rigidizing Overtube, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.

.jpg "Marina Kim, DO (she/her/hers) photo")