P4359 - Long-Term Efficacy and Safety of Intravenous (IV) Tulisokibart in Patients With Ulcerative Colitis (UC): Results From the Open-Label Extension (OLE) Period of the Phase 2 ARTEMIS-UC Study
Icahn School of Medicine at Mount Sinai New York, NY
Christopher Ma, MD1, Sami Hoque, MD2, Miles P.. Sparrow, MD3, Jaclyn K.. Anderson, DO4, Mark Yen, MD4, Bin Dong, PhD4, Brian G.. Feagan, MD5, Bruce E.. Sands, MD, FACG6 1University of Calgary, Calgary, AB, Canada; 2Barts Health NHS Trust, London, England, United Kingdom; 3School of Translational Medicine, Monash University and Alfred Health, Melbourne, VIC, Australia, Melbourne, Victoria, Australia; 4Merck & Co., Inc., Rahway, NJ; 5Western University, London, ON, Canada; 6Icahn School of Medicine at Mount Sinai, New York, NY
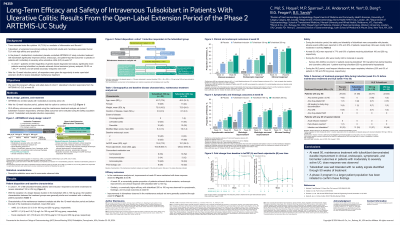
Introduction: Tumor necrosis factor–like cytokine 1A (TL1A) is a regulator of inflammation and fibrosis in inflammatory bowel disease. Tulisokibart, an anti-TL1A monoclonal antibody, demonstrated efficacy without clinically meaningful safety findings vs placebo after a 12-week induction in adults with moderately to severely active UC in the multicenter, double-blind, placebo-controlled phase 2 ARTEMIS-UC study. We report long-term efficacy and safety of tulisokibart among cohort 1 induction responders at week 50 from the OLE period of ARTEMIS-UC.
Methods: Cohort 1 of ARTEMIS-UC enrolled participants regardless of genetic-based diagnostic test status. After the 12-week induction period, in which randomized participants received IV tulisokibart (1000 mg on day 1; 500 mg at weeks 2, 6, 10) or placebo, participants had the option to continue in the OLE. Participants were classified as induction responders (defined as reduction of ≥2 points and ≥30% in modified Mayo score from baseline with a reduction ≥1 in rectal bleeding [RB] subscore or absolute RB subscore ≤1 at week 12) or induction nonresponders. Cohort 1 induction responders in the tulisokibart group were randomized to receive open-label IV tulisokibart 100 or 250 mg Q4W at 14–170 weeks. Efficacy outcomes are reported for induction responders from the tulisokibart group. Safety is reported for induction responders from tulisokibart and placebo groups. Descriptive statistics were used to summarize observed data.
Results: 47 cohort 1 induction responders in the tulisokibart group were randomized to receive tulisokibart 250 mg (n=25) or 100 mg (n=22). Improvements in clinical, endoscopic, and biomarker outcomes observed with tulisokibart were generally maintained through week 50 in both dose groups (Table). A greater proportion of patients achieved clinical and endoscopic outcomes with tulisokibart 250 vs 100 mg. In the safety population, (tulisokibart 250 mg, n=35; 100 mg, n=30), through week 50, AEs occurred in 63% and 77% of participants receiving tulisokibart 250 and 100 mg, respectively; most were mild to moderate in severity. Serious AEs occurred in 1 (3%) and two (7%) participants in the tulisokibart 250 and 100 mg groups, respectively.
Discussion: At week 50, maintenance of treatment effect was generally observed in cohort 1 induction responders. A trend for higher efficacy with tulisokibart 250 vs 100 mg was observed. Tulisokibart was well tolerated with no identified safety signals. Larger trials are needed to confirm these findings.
Note: The table for this abstract can be viewed in the ePoster Gallery section of the ACG 2024 ePoster Site or in The American Journal of Gastroenterology's abstract supplement issue, both of which will be available starting October 27, 2024.
Christopher Ma, MD1, Sami Hoque, MD2, Miles P.. Sparrow, MD3, Jaclyn K.. Anderson, DO4, Mark Yen, MD4, Bin Dong, PhD4, Brian G.. Feagan, MD5, Bruce E.. Sands, MD, FACG6. P4359 - Long-Term Efficacy and Safety of Intravenous (IV) Tulisokibart in Patients With Ulcerative Colitis (UC): Results From the Open-Label Extension (OLE) Period of the Phase 2 ARTEMIS-UC Study, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.