Analine B.. Delgado, BS1, Madeline Sesselmann, DO1, Zbigniew Malecki, MD2, Faris Murad, MD1 1Advocate Lutheran General, Park Ridge, IL; 2Advocate Illinois Masonic Medical Center, Chicago, IL
Introduction: Urothelial carcinoma (UC) affects the urinary tract and is the most common form of bladder cancer. UC rarely metastasizes to distant sites, but has been documented in approximately 4% of patients. Gastrointestinal involvement, notably gastric metastasis, is an exceptionally uncommon manifestation. We report the case of urothelial carcinoma metastasizing to the stomach, presenting as a large gastric mass.
Case Description/Methods: An 82-year-old male with a history of high grade non-muscle invasive bladder cancer, prostate cancer, and chronic anemia presented with increased chest pain and dyspnea. He was treated with BCG immunotherapy for his bladder cancer a decade prior to presentation, and his recent cystoscopy was unremarkable. CTA identified an infiltrative mass in the posterior left upper lobe and pathologic fractures of multiple ribs and T3. Lung biopsy indicated a high-grade malignant neoplasm, favoring a urothelial primary.
He was referred to GI due to an abnormal PET/CT scan which showed a hypermetabolic lung mass, mildly hypermetabolic mediastinal/hilar lymph nodes, and focal hypermetabolic activity in the stomach concerning neoplasm. Subsequent EGD revealed a large, fungating, infiltrative, and ulcerated mass on the greater curvature of the stomach. Immunohistochemical staining showed tumor cells positive for GATA3, uroplakin, p63, and CK7, and negative for CDX2, CK20, CD56, chromogranin, PSAP, synaptophysin, NKX3.1 supporting the diagnosis of a primary urothelial carcinoma.
Interestingly, the patient had undergone upper endoscopy a year prior due to worsening anemia and blood in stools, but showed only superficial gastric ulcers and H. pylori infection, with no malignancy detected at the time.
Discussion: The pathogenesis of gastric metastasis from urothelial carcinoma is not well understood, but dissemination likely involves hematogenous spread. The most common sites of metastatic UC include lymph nodes, lung, liver, and bone. Our patient had a recent negative cystoscopy, and presented without GI symptoms. He was admitted a year prior due to worsening anemia. Evaluation on upper endoscopy at the time showed no signs of malignancy. This case demonstrates that although uncommon, UC may metastasize to unusual sites including the stomach. The progression suggests a rapid metastatic spread, emphasizing the need for continuous vigilance in patients with a history of urothelial carcinoma, even in the absence of recent diagnostic evidence of disease spread.
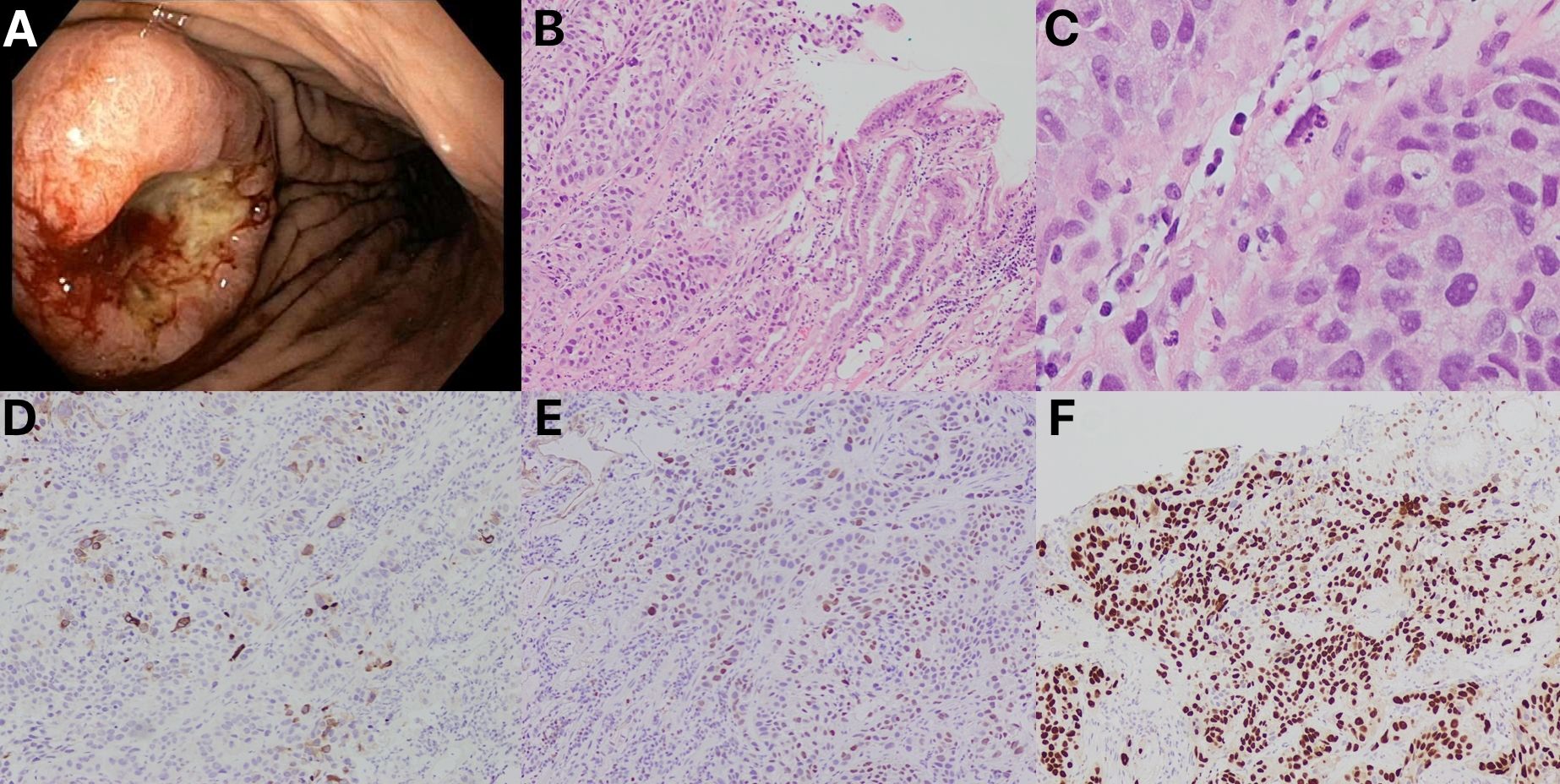
Figure: Figure 1. An 82-year-old male underwent an endoscopy for an abnormal PET/CT scan of the GI tract and was found to have a large, fungating, infiltrative, and ulcerated non-circumferential mass on the greater curvature of the stomach. The endoscopy image shows a malignant gastric tumor that was biopsied with cold forceps for histology (A). H&E stains demonstrate gastric mucosa with stromal nests of anaplastic epithelial cells (B, C). Positive uroplakin II (D), GATA 3 (E), and p63 (F) stains were observed. The morphologic and immunohistochemical stains are consistent with a diagnosis of metastatic urothelial carcinoma.
Disclosures:
Analine Delgado indicated no relevant financial relationships.
Madeline Sesselmann indicated no relevant financial relationships.
Zbigniew Malecki indicated no relevant financial relationships.
Faris Murad indicated no relevant financial relationships.
Analine B.. Delgado, BS1, Madeline Sesselmann, DO1, Zbigniew Malecki, MD2, Faris Murad, MD1. P5081 - Metastatic Urothelial Carcinoma Presenting as Gastric Mass, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.


 photo")