Jordan Carty, MD1, Tara John, MBBS1, Otoniel Ysea Hill, MD1, Jessica Genkil, DO2, Nandakumar Mohan, DO3, Zurab Azmaiparashvili, MD, MSc4, Maria Lagarde Mussa, MD5 1Albert Einstein Medical Center, Philadelphia, PA; 2Jefferson Einstein, Huntingdon Valley, PA; 3Einstein Healthcare Network, Philadelphia, PA; 4Jefferson Einstein Hospital, Philadelphia, PA; 5Einstein Medical Center, Philadelphia, PA
Introduction: Cutaneous caput medusae bleeding is a rare, life-threatening complication of portal hypertension. Due to limited cases, no definitive treatment exists. We present a case treated with transjugular intrahepatic portosystemic shunt (TIPS).
Case Description/Methods: A 49-year-old man with a history of alcohol and cocaine abuse, presented with abdominal wall bleeding for four days. He was slightly tachycardic but otherwise hemodynamically stable. Physical examination was significant for lethargy, scleral icterus, and bleeding abdominal wall caput medusae. Initial work-up showed a hemoglobin level 5.5 g/dl, platelet count 256 x 10^3/µL, creatinine 0.98 mg/dl, AST 239 IU/L, ALT 112 IU/L, total bilirubin 3.7 mg/dl, direct bilirubin 2.1 mg/dl, albumin 1.9 g/dl, INR 1.7, lactic acid 6.80 mmol/L, AFP 150 ng/ml (0-10) and MELD 28
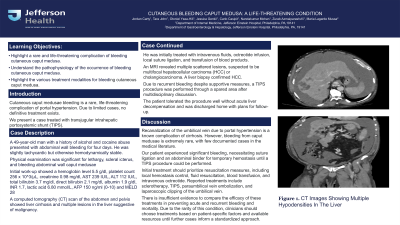
A computed tomography (CT) scan of the abdomen and pelvis showed liver cirrhosis and multiple lesions in the liver suggestive of malignancy. He was initially treated with intravenous fluids, octreotide infusion, local suture ligation, and transfusion of blood products. An MRI revealed multiple scattered lesions, suspected to be multifocal hepatocellular carcinoma (HCC) or cholangiocarcinoma. A liver biopsy confirmed HCC. Due to recurrent bleeding despite supportive measures, a TIPS procedure was performed through a spared area after multidisciplinary discussion. The patient tolerated the procedure well without acute liver decompensation and was discharged home with plans for follow-up.
Discussion: Recanalization of the umbilical vein due to portal hypertension is a known complication of cirrhosis. However, bleeding from caput medusae is extremely rare, with few documented cases in medical literature. Our patient experienced significant bleeding, necessitating suture ligation and an abdominal binder for temporary hemostasis until a TIPS procedure could be performed.
Initial treatment should prioritize resuscitation measures, including local hemostasis control, fluid resuscitation, blood transfusion, and intravenous octreotide. Reported treatments include sclerotherapy, TIPS, paraumbilical vein embolization, and laparoscopic clipping of the umbilical vein. There is insufficient evidence to compare the efficacy of these treatments in preventing acute and recurrent bleeding and mortality. Due to the rarity of this condition, clinicians should choose treatments based on patient-specific factors and available resources until further cases inform a standardized approach.
Disclosures:
Jordan Carty indicated no relevant financial relationships.
Tara John indicated no relevant financial relationships.
Otoniel Ysea Hill indicated no relevant financial relationships.
Jessica Genkil indicated no relevant financial relationships.
Nandakumar Mohan indicated no relevant financial relationships.
Zurab Azmaiparashvili indicated no relevant financial relationships.
Maria Lagarde Mussa indicated no relevant financial relationships.
Jordan Carty, MD1, Tara John, MBBS1, Otoniel Ysea Hill, MD1, Jessica Genkil, DO2, Nandakumar Mohan, DO3, Zurab Azmaiparashvili, MD, MSc4, Maria Lagarde Mussa, MD5. P4759 - Cutaneous Bleeding Caput Medusa: A Life-Threatening Condition, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.