New York Medical College - Saint Michael's Medical Center Newark, NJ
Mohammad N. Kloub, MD1, Byron Okwesili, MD1, Mohammad Abushanab, MD1, Ahmad Haddad, MD1, Atheer Anwar, MD2, Qusai Al-maharmeh, MD1, Raed Atiyat, MD1, Theodore DaCosta Jr, MD1 1New York Medical College - Saint Michael's Medical Center, Newark, NJ; 2Mutah University, Newark, NJ
Introduction: Charcot-Marie-Tooth Disease Is an inherited degenerative disease affecting the peripheral nervous system, causing motor and sensory neuropathy and distal muscle atrophy. The disease is slowly progressive and can affect proximal muscle lately. Involvement of smooth muscles like the diaphragm and esophagus is extremely rare. We present a male patient with advanced Charcot-Marie-Tooth Disease who was admitted to the hospital with aspiration pneumonia and found to have esophageal dysmotility.
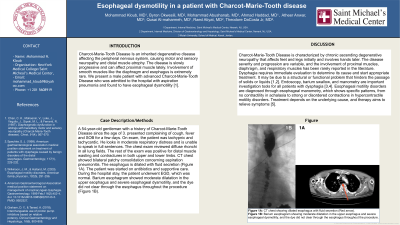
Case Description/Methods: A 54-year-old gentleman with a history of Charcot-Marie-Tooth Disease since the age of 3. presented complaining of cough, fever and SOB for a few days. On exam, the patient was tachypnic and tachycardic. He looks in moderate respiratory distress and is unable to speak in full sentences. The chest exam reviewed diffuse rhonchi in all lung fields. The rest of the exam was positive for distal muscle wasting and contractures in both upper and lower limbs. CT chest showed bilateral patchy consolidation concerning aspiration pneumonitis. The esophagus is dilated with fluid secretion (Figure 1A). The patient was started on antibiotics and supportive care. During the hospital stay, the patient underwent EGD, which was normal. Barium esophagram showed moderate dilatation in the upper esophagus and severe esophageal dysmotility, and the dye did not clear through the esophagus throughout the procedure (Figure 1B).
Discussion: Charcot-Marie-Tooth Disease is characterized by chronic ascending degenerative neuropathy that affects feet and legs initially and involves hands later. The disease severity and progression are variable, and the involvement of proximal muscles, diaphragm, and respiratory muscles has been rarely reported in the literature. Dysphagia requires immediate evaluation to determine its cause and start appropriate treatment. It may be due to a structural or functional problem that hinders the passage of solids or liquids. Esophageal dysmotility strikes when the esophagus muscles fail to contract normally, leading to difficulty swallowing. Endoscopy, barium swallow, and manometry are important investigation tools for all patients with dysphagia. Esophageal motility disorders are diagnosed through esophageal manometry, which shows specific patterns, from no contractility in achalasia to strong or disordered contractions in hypercontractile motility disorders. Treatment depends on the underlying cause, and therapy aims to relieve symptoms.
Figure: Figure 1A: CT chest showing dilated esophagus with fluid secretion (Red arrow). Figure 1B: Barium esophagram showing moderate dilatation in the upper esophagus and severe esophageal dysmotility, and the dye did not clear through the esophagus throughout the procedure.
Disclosures:
Mohammad Kloub indicated no relevant financial relationships.
Byron Okwesili indicated no relevant financial relationships.
Mohammad Abushanab indicated no relevant financial relationships.
Ahmad Haddad indicated no relevant financial relationships.
Atheer Anwar indicated no relevant financial relationships.
Qusai Al-maharmeh indicated no relevant financial relationships.
Raed Atiyat indicated no relevant financial relationships.
Theodore DaCosta Jr indicated no relevant financial relationships.
Mohammad N. Kloub, MD1, Byron Okwesili, MD1, Mohammad Abushanab, MD1, Ahmad Haddad, MD1, Atheer Anwar, MD2, Qusai Al-maharmeh, MD1, Raed Atiyat, MD1, Theodore DaCosta Jr, MD1. P3986 - Esophageal Dysmotility in a Patient With Charcot-Marie-Tooth Disease, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.


 photo")
