Danielle Tran, BS1, Ariana R. Tagliaferri, MD2, Kayvon Sotoudeh, MD2, Savio Reddymasu, MBBS, FACG2 1Creighton University School of Medicine, Omaha, NE; 2Creighton University Medical Center, Phoenix, AZ
Introduction: The risk of pancreatic cancer in patients with Lynch syndrome is 3.68% and includes variants of ductal adenocarcinoma, such as medullary or colloid types. Medullary carcinomas are associated with microsatellite instability (MSI) accounting for their presence with Lynch syndrome; a condition due to mutations in mismatch repair proteins (MMR) leading to MSI. Colloid carcinoma is derived from IPMN’s or mucinous cystic neoplasms and there are only a few cases per 1 million annually. Pancreatic colloid carcinoma is microsatellite stable and rarely occurs concomitantly with Lynch syndrome.
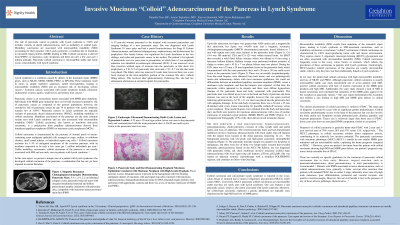
Case Description/Methods: A 57-year-old-woman with Lynch syndrome and colon cancer s/p hemicolectomy 8 years prior presented with acute pancreatitis. 2 years prior, a 2cm ampullary polyp, negative for dysplasia or malignancy was removed via en-bloc resection. On arrival, lipase was >4,000 and MRCP showed pancreatic duct dilation of 7mm with a septate cystic mass in the body. CA 19-9 was 189 units/mL. An EUS and ERCP revealed a 25mm x 20mm hypoechoic lesion in the pancreatic body, a 20mm x 20mm multicystic lesion in the pancreatic head, without lymphadenopathy. A distal biliary stricture was dilated to 6mm. A 10Fr x 7cm plastic biliary stent was placed. Diffuse hyperechoic changes of the pancreatic head and body were indicative of pancreatitis. FNB’s obtained from the body, tail and pancreatic duct were positive for mucinous adenocarcinoma with a loss of nuclear expression of MMR proteins MLH1/PMS2. She had a total pancreatectomy, hepaticojejunostomy, gastrojejunostomy and cholecystectomy. The resected pancreas body and tail demonstrated multifocal invasive mucinous colloid adenocarcinoma with focal signet ring cell features (pT3 pN2 cM0). The largest focus in the distal pancreas measured 14cm. The background pancreas had low-grade and high-grade intraepithelial neoplasia from an IPMN. She started adjuvant chemotherapy with a modified FOLFIRINOX regimen and currently follows with Oncology.
Discussion: Colloid carcinoma and concomitant Lynch syndrome is reported in the ovary, colon, breast or stomach due to mucin-2 oligomeric glycoprotein (MUC2) which causes MSI’s. Conversely, MUC2 pancreatic colloid carcinomas are microsatellite stable and thus are rarely seen with Lynch syndrome. Our case features a rare pancreatic cancer, which is also rarely associated with Lynch syndrome. Moreover, her colloid-type carcinoma expressed a genetic phenotype not typically seen, characterized by high MSI and loss of MMR genes.
Disclosures:
Danielle Tran indicated no relevant financial relationships.
Ariana Tagliaferri indicated no relevant financial relationships.
Kayvon Sotoudeh indicated no relevant financial relationships.
Savio Reddymasu indicated no relevant financial relationships.
Danielle Tran, BS1, Ariana R. Tagliaferri, MD2, Kayvon Sotoudeh, MD2, Savio Reddymasu, MBBS, FACG2. P3587 - Invasive Mucinous “Colloid” Adenocarcinoma of the Pancreas in Lynch Syndrome, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.


 photo")