P4398 - The Impact of Mirikizumab Induction, Maintenance, and Long-Term Treatment on Disease Clearance in Patients With Moderately to Severely Active Ulcerative Colitis: Post-Hoc Analysis of LUCENT Trials
Jean-Frédéric Colombel, MD1, Taku Kobayashi, MD2, Jianmin Wu, 3, Baojin Zhu, 3, Vipul Jairath, MBChB4, Isabel Redondo, MD5, Richard Moses, 3, Corey A.. Siegel, MD, MS6, Britta Siegmund, MD7, Fernando Magro, 8 1Icahn School of Medicine at Mount Sinai, New York, NY; 2Kitasato University Kitasato Institute Hospital, Minato City, Tokyo, Japan; 3Eli Lilly and Company, Indianapolis, IN; 4Western University, London, ON, Canada; 5Eli Lilly and Company, Lisboa, Lisboa, Portugal; 6Dartmouth-Hitchcock Medical Center, Lebanon, NH; 7Med. Klinik für Gastroenterologie, Infektiologie, Rheumatologie, Charité – Universitätsmedizin Berlin, Freie Universität Berlin, Humboldt-Universität zu Berlin, Campus Benjamin Franklin, Hindenburgdamm, Berlin, Germany; 8Centro Hospitalar São João, Porto, Porto, Portugal
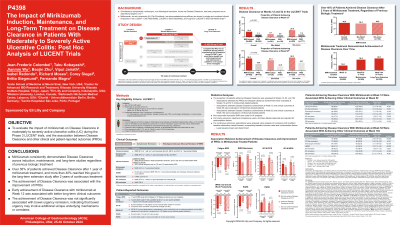
Introduction: Disease clearance (DC) has been proposed as an aspirational target in ulcerative colitis (UC). Mirikizumab (miri) has demonstrated strong efficacy in LUCENT Phase 3 trials. This analysis evaluated the impact of miri on DC during LUCENT-1, -2 and long-term LUCENT-3 trials and the association between DC and other clinical and patient-reported outcomes (PROs).
Methods: DC: symptomatic remission [Mayo stool frequency (SF)=0, 1 with ≥1 point decrease from baseline + rectal bleeding (RB)=0] and histologic-endoscopic mucosal remission [HEMR: Mayo endoscopic remission (ER: endoscopy subscore of 0 or 1, excluding friability) + Geboes score ≤2B.0]. PROs: Fatigue NRS, IBDQ remission, SF-36, WPAI:UC, PGRS and PGRC (see table footer). Clinical outcomes: clinical remission, corticosteroid-free remission, ER, HEMR, bowel urgency (BU) remission, SF remission and RB remission. Patient proportion achieving DC was assessed at W12, 52 and 104. Associations between the PROs and DC were evaluated at W12 and 52 and those between clinical outcomes and early DC achievement in miri-treated patients at W12 and W52 were evaluated at W52 and W104, respectively.
Results: Significantly higher proportion of miri-treated patients achieved DC vs PBO at W12 (N=868 miri, 294 PBO; DC: 16.0% vs 7.1%, p< 0.0001) and W52 (N=365 miri, 179 PBO; DC: 36.4% vs 19.6%, p=0.0002). Similar trends were seen for biologic failure subgroups at W12 (bio/JAKi-failed DC: 9.1% miri vs 5.9% PBO; bio&JAKi-naïve DC: 20.9% miri vs 7.6% PBO) and W52 (bio/JAKi-failed DC: 31.3% miri vs 12.5% PBO; bio&JAKi-naïve DC: 39.3% miri vs 23.7% PBO). At W104 (N=239 miri), 40.6% patients achieved DC with 2-year of treatment. 38.4% bio/JAKi-failed (n=73) and 40.9% bio&JAKi-naïve (n=159) patients achieved DC. Significantly greater improvement in all PROs was seen at W12 for miri-treated patients who achieved DC vs those who did not at W12. Similar associations were observed at W52, except in WPAI: UC overall work productivity (Table-1A). Patients achieving DC at W12 were more likely to achieve all clinical outcomes, except BU remission, at W52 vs those who did not achieve W12 DC. This trend repeated in those who achieved DC at W52 and continued to W104 (Table-1B).
Discussion: Miri consistently demonstrated DC across induction, maintenance and long-term studies. Over 36% patients achieved DC after one year of miri treatment. DC attainment was associated with improvement in PROs in LUCENT-1 and -2. Early DC was associated with better long-term clinical outcomes.
Note: The table for this abstract can be viewed in the ePoster Gallery section of the ACG 2024 ePoster Site or in The American Journal of Gastroenterology's abstract supplement issue, both of which will be available starting October 27, 2024.