Ibukunoluwa Oshobu, MD1, Mustafa Gandhi, MD1, Ryan Jobe, MD2, Murtaza Gandhi, MBBS3, Yezaz Ghouri, MD4 1University of Missouri Health Care, Columbia, MO; 2University of Missouri School of Medicine, Gainesville, FL; 3Terna Medical College, Columbia, MO; 4University of Missouri School of Medicine, Columbia, MO
Introduction: Deglutition syncope is a reflex syncope triggered by swallowing. Swallowing causes esophageal dilation, stimulating vagal afferents. This leads to an exaggerated parasympathetic response in cardiac vagal efferents, resulting in life-threatening hypotension and bradyarrhythmia, causing syncope due to cerebral hypoperfusion.
Case Description/Methods: A 66-year-old female with reflux esophagitis, hiatal hernia, and deglutition syncope presented for her 4thesophagogastroduodenoscopy (EGD). She had undergone controlled radial expansion (CRE) balloon dilation twice without complications. When a CRE balloon was dilated from 6mm to 8mm over a critical stricture at the gastroesophageal junction, the patient had bradycardia, which deteriorated into a complete heart block, necessitating scope withdrawal. Subsequently, the heart rate and rhythm normalized. Upon introducing a new endoscope at the mid-esophagus, the patient developed a complete heart block, prompting immediate procedure termination. A tilt table test was positive for vasodepressor pre-syncope, and telemetry findings were consistent with intermittent complete heart block. The echocardiogram revealed normal findings with trivial mitral regurgitation. The patient then underwent elective implantation of a leadless MICRA pacemaker. Deglutition-related syncopal symptoms resolved after pacemaker implantation. Stricture dilation 1 year later did not cause bradyarrhythmia.
Discussion: Deglutition syncope, strongly linked to gastrointestinal (GI) disease (hiatal hernia, achalasia, and esophageal strictures) requires a detailed history, Holter/event monitors, and tilt-table tests for diagnosis. Cardiac imaging, ECG, and EGD help to identify underlying disorders. Exaggerated vagal activation during swallowing likely causes a cardioinhibitory response that may be reversed with atropine. Treatment of underlying GI disease may resolve symptoms. However, repeated dilations in this case worsened syncopal symptoms, causing heart block, and necessitating pacemaker placement for treatment. Previously tolerating 3 previous EGDs without complications, points to the sudden nature of this adverse event. When the balloon was deflated at the GEJ stricture, the bradyarrhythmia resolved to suggest that the mechanoreceptors in the lower esophagus played a role in this mechanism.
Awareness of deglutition syncope's association with lethal bradyarrhythmia from esophageal dilation or EGD is crucial for preventing morbidity and mortality.
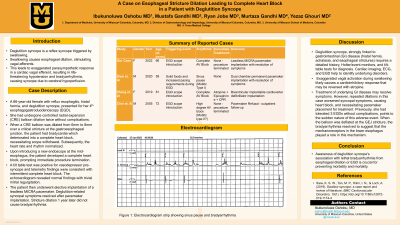
Figure: Electrocardiogram strip showing sinus pause and bradyarrhythmia.
Note: The table for this abstract can be viewed in the ePoster Gallery section of the ACG 2024 ePoster Site or in The American Journal of Gastroenterology's abstract supplement issue, both of which will be available starting October 27, 2024.
Disclosures:
Ibukunoluwa Oshobu indicated no relevant financial relationships.
Mustafa Gandhi indicated no relevant financial relationships.
Ryan Jobe indicated no relevant financial relationships.
Murtaza Gandhi indicated no relevant financial relationships.
Yezaz Ghouri indicated no relevant financial relationships.
Ibukunoluwa Oshobu, MD1, Mustafa Gandhi, MD1, Ryan Jobe, MD2, Murtaza Gandhi, MBBS3, Yezaz Ghouri, MD4. P3997 - A Case of Esophageal Stricture Dilation Leading to Complete Heart Block in a Patient With Deglutition Syncope, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.

 photo")
