University of Oklahoma Health Sciences Center Oklahoma City, OK
Luke Sorensen, MD1, Satya Sai Venkata Lakshmi Arepalli, MD1, Katherine Janike, MD2, Andrea Fernandez, MD1, Javid Fazili, MD1 1University of Oklahoma Health Sciences Center, Oklahoma City, OK; 2University of Oklahoma College of Medicine, Oklahoma City, OK
Introduction: Meckel's diverticulum (MD) is the most common congenital abnormality of the GI tract, seen in 1-3% of general population, resulting from incomplete atresia of the vitelline duct [1,2]. Although typically asymptomatic, there is a 4-6% lifetime risk of developing bleeding, obstruction and diverticulitis with 40% of these symptoms found in patients under 10 years old [3-4]. Given complications decrease with age, diagnosis of MD in adults is often incidental.
Case Description/Methods: A 19-year-old woman with Cornelia-de-lange syndrome (on therapeutic warfarin) and recurrent GI bleeding presented with melena. Previously, she has had extensive work up including EGD, balloon assisted enteroscopy, VCE, colonoscopy, and a Meckel’s scan. All exams were essentially unremarkable. During a previous admission for GI bleed, a CTA of the abdomen and pelvis found active bleeding from the jejunal artery and was embolized by IR. Unfortunately, she later developed hemorrhagic shock and was taken for an explorative laparotomy. MD was found to be the source of bleeding, confirmed with intraoperative fluoroscopy. She underwent resection of the MD and was stable post operatively. Histology report reaffirmed the diagnosis with the presence of ectopic gastric tissue. To date, she has not had further GI bleeding even after reinitiating anticoagulation.
Discussion: MD in adults, if symptomatic, will typically present as intestinal obstruction (22-50%) or diverticulitis/perforation (20%) [5]. Though GI bleeds are seen in children, there are only a few case reports describing hemorrhagic shock in adults. The exact cause of GI bleeding is thought to be due to the acid created by the ectopic gastric mucosa leading to ulceration and bleeding. Typically, the acid produced in the GI tract is neutralized by bicarbonate secreted from the pancreas. In MD, the ileal outpouching encloses the acid allowing it to degrade the mucosa [5]. We suspect this patient’s presentation was exacerbated by her therapeutic anticoagulation making her more susceptible to hemorrhage. MD is usually diagnosed in children using technetium-99m pertechnetate scanning. However, in adults the sensitivity and specificity are 62% and 9% respectively, leading to many false results and the cause of our patient’s late diagnosis [6]. Although rare, this can be a life-threatening condition that might require emergent surgery and therefore vital to include in differentials with recurrent GI bleeds.
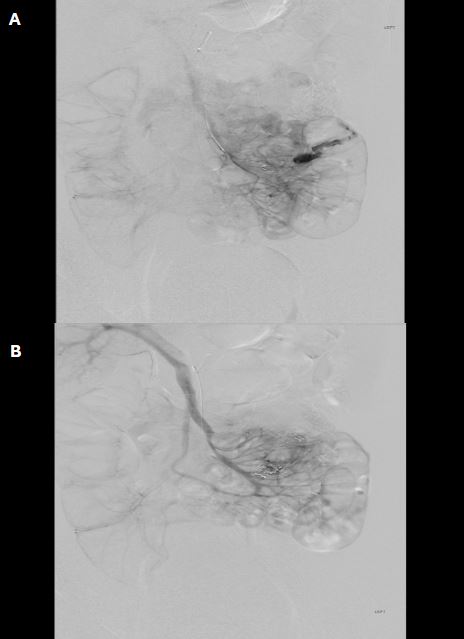
Figure: A) Angiographic image demonstrating area of extravasation of contrast in the left lower quadrant near a previously placed coil. B) Angiographic image demonstrating the absence of extravasation of contrast after 2mm Boston Scientific Embold coils were placed in two of the sub-selective branches of the ileal artery.
Disclosures:
Luke Sorensen indicated no relevant financial relationships.
Satya Sai Venkata Lakshmi Arepalli indicated no relevant financial relationships.
Katherine Janike indicated no relevant financial relationships.
Andrea Fernandez indicated no relevant financial relationships.
Javid Fazili indicated no relevant financial relationships.
Luke Sorensen, MD1, Satya Sai Venkata Lakshmi Arepalli, MD1, Katherine Janike, MD2, Andrea Fernandez, MD1, Javid Fazili, MD1. P4225 - Meckel’s Diverticulum: A Cause of Unknown Hemorrhagic Shock, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.