Dipam Shah, MD1, Ussama Ghumman, MD2, Kathryn Hobbs, MD1, Lawrence Istrail, MD3 1Inova Fairfax Medical Campus, Fairfax, VA; 2Bayhealth Medical Center, Dover, DE; 3Inova Fairfax Medical Campus, Falls Church, VA
Introduction: Upper gastrointestinal bleeding (UGIB) is a gastroenterological (GI) emergency with a mortality rate of 6% to 13%. Despite changes in management, mortality has not significantly improved over the last 50 years. Esophagogastroduodenoscopy (EGD) is the gold standard for diagnosis of UGIB, however, there is scant literature exploring the role of point-of-care ultrasound (POCUS) in the diagnosis of UGIB.
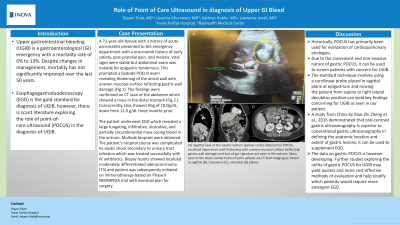
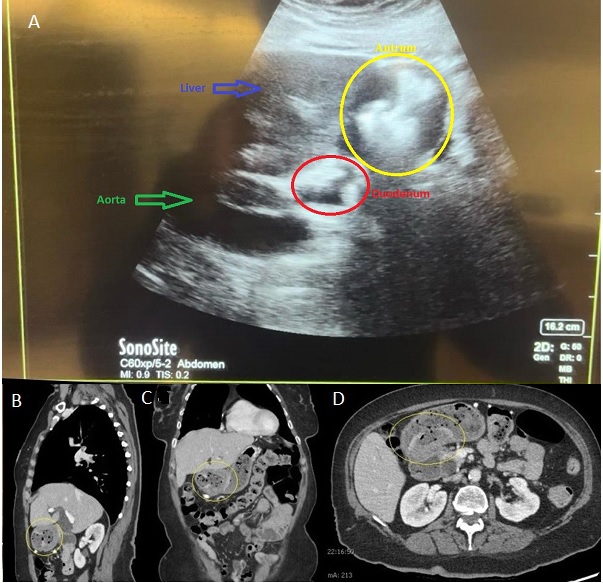
Case Description/Methods: A 71-year-old female with a history of acute pancreatitis presented to the emergency department with a one-month history of early satiety, post-prandial pain, and melena. Vital signs were stable but abdominal exam was notable for epigastric tenderness. This prompted a bedside POCUS exam revealing thickening of the antral wall with uneven mucosal surface reflecting gastric wall damage (Fig 1). The findings were confirmed on CT scan of the abdomen which showed a mass in the distal stomach (Fig 2.). Concurrently, labs showed Hbg of 10.0g/dL, down from 12.0 g/dL three months prior.
The patient underwent EGD which revealed a large fungating, infiltrative, ulcerative, and partially circumferential mass oozing blood in the antrum. Multiple biopsies were obtained. The patient’s hospital course was complicated by septic shock secondary to urinary tract infection which was treated successfully with IV antibiotics. Biopsy results showed localized moderately differentiated adenocarcinoma (T3) and patient was subsequently initiated on immunotherapy based on Phase II NEONIPIGA trial with eventual plan for surgery.
Discussion: Historically, POCUS has primarily been used for evaluation of cardiopulmonary etiologies. Due to the convenient and non-invasive nature of gastric POCUS, it can be used to screen patients with concern for UGIB. The standard technique involves using a curvilinear probe placed in sagittal plane at epigastrium and moving the patient from supine to right lateral decubitus position can yield key findings concerning for UGIB as seen in our patient. A study from China by Xiao-Zhi Zheng et al., 2016 demonstrated that oral-contrast gastric ultrasonography is superior to conventional gastric ultrasonography in defining the anatomic location and extent of gastric lesions; it can be used to supplement EGD. The data on gastric POCUS is however developing. Further studies exploring the utility of gastric POCUS for UGIB may yield quicker and more cost-effective methods of evaluation and help stratify which patients would require more emergent EGD.
Figure: (A) Sagittal view of the Gastric antrum (yellow circle) obtained on POCUS. Localized hypoechoic wall thickening with uneven mucosal surface (reflecting gastric wall damage) and loss of gut signature are seen in the antrum. Mass seen in the distal stomach (encircled in yellow) via CT Scan imaging as shown in sagittal (B), transverse (C), and axial (D) planes.
Disclosures:
Dipam Shah indicated no relevant financial relationships.
Ussama Ghumman indicated no relevant financial relationships.
Kathryn Hobbs indicated no relevant financial relationships.
Lawrence Istrail indicated no relevant financial relationships.
Dipam Shah, MD1, Ussama Ghumman, MD2, Kathryn Hobbs, MD1, Lawrence Istrail, MD3. P4226 - Role of Point of Care Ultrasound in Diagnosis of Upper GI Bleed, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.