Paxton Smith, MD1, Nishant Puri, MD, FACG2 1Providence Sacred Heart Medical Center, Cheney, WA; 2Providence Sacred Heart Medical Center, Spokane, WA
Introduction: Prostate cancer typically metastasizes to bones and lymph nodes. Metastasis to the gastrointestinal system is very rare with only 16 cases of gastric metastasis reported in the literature. We report on the endoscopic features of gastric metastasis from prostate cancer.
Case Description/Methods: A 67-year-old male with prostate cancer developed metastasis to his bladder and colon that were treated with radiation and androgen deprivation therapy. Further metastases were identified in his kidneys and lymph nodes, and he underwent further radiation and treatment with Enzalutamide. After 14 months, he complained of new onset upper back pain and heartburn concerning for gastroesophageal reflux disease. A restaging positron emission tomogram (PET) scan showed new areas of enhancement in the gastric fundus and cardia. An upper endoscopy demonstrated Los Angeles grade D esophagitis and diffuse erythema of the gastric body, which was biopsied. Pathology was consistent with adenocarcinoma, originating from the prostate. Immunohistochemical staining was positive for NKX3.1 which carries a high 98.6% sensitivity and 99% specificity for prostate cancer.
Discussion: Metastatic prostate cancer portends a poor prognosis with significant morbidity and mortality. It typically metastasizes to the bones, lymph nodes, and liver. Metastasis to the stomach is extremely rare with only 16 cases reported in the literature. This patient had upper back pain, reflux and increased uptake on a PET scan in the gastric fundus and cardia. Conventionally, gastric metastasis is often described as a depressed area or a discrete tumor. However, our patient had diffuse erythema without discrete nodularity. This case adds to the increasing number of cases of prostate cancer metastasizing to the GI tract, and the different ways in which it may present, which may help guide further management and diagnostic accuracy. Due to the aggressive nature of his cancer his oncology team transitioned him from his Enzalutamide to Lutetium vipivotide tetraxetan.
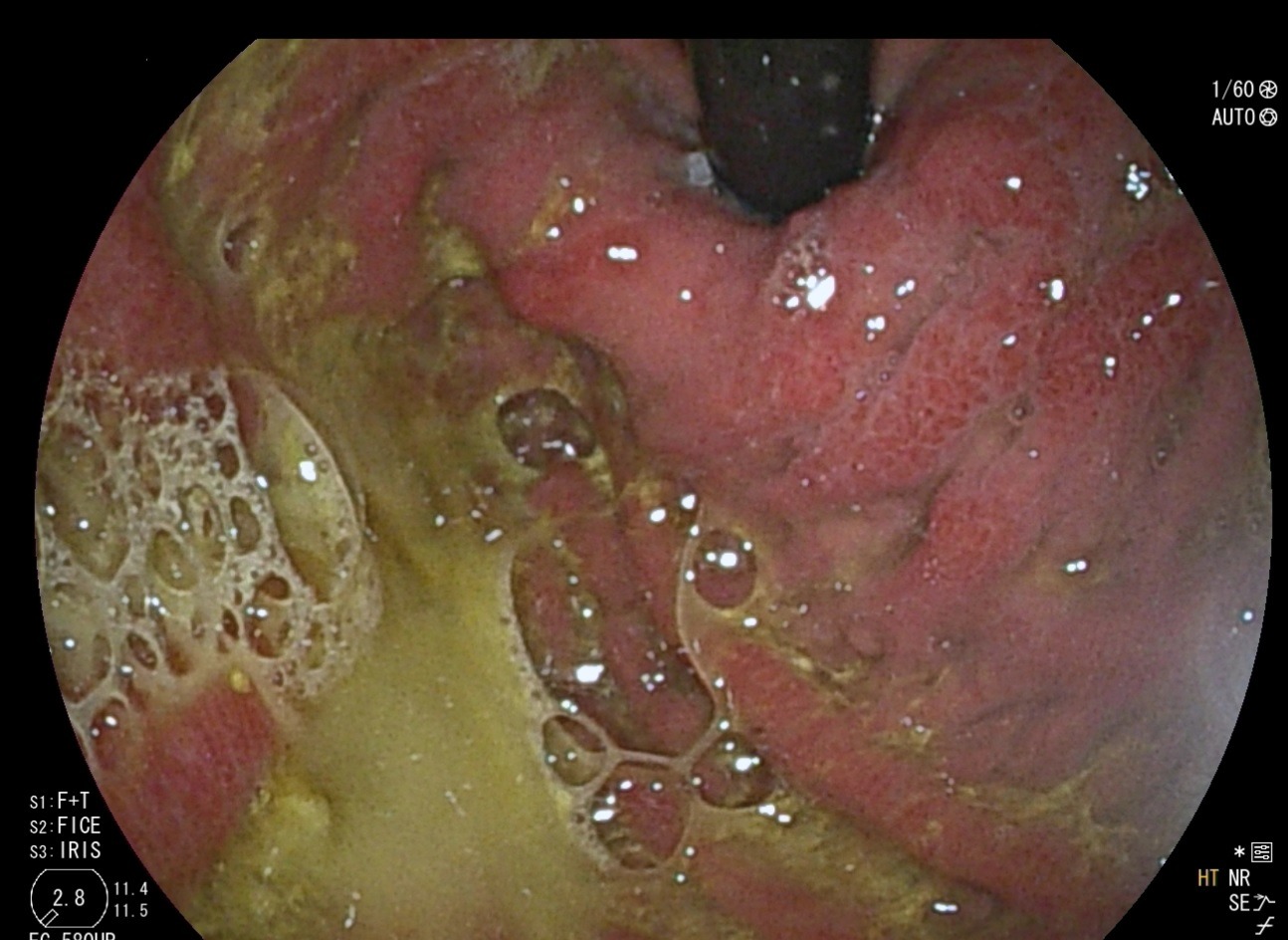
Figure: Gastric mucosa showing erythema.
Disclosures:
Paxton Smith indicated no relevant financial relationships.
Nishant Puri: Boston Scientific – Consultant.
Paxton Smith, MD1, Nishant Puri, MD, FACG2. P4146 - Rare Manifestation of Prostate Cancer in the Stomach, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.