Deenanath Mangeshkar Hospital and Research Center Pune, Maharashtra, India
Yash Kanani, MBBS, MD1, Chetan Oswal, Mbbs, MD1, Sanjana Bhagwat, MBBS, MD1, Chaitaniya Kumbhar, MBBS, MD1, Arun Arora Pagadapelli, MBBS1, Amit Daphale, MBBS2, Sachin Palnitkar, MBBS, MD, DM1, Rajendra Pujari, MBBS, MD, MRCP1, Harshal Gadhikar, MBBS, MD, DM1, Amol Bapaye, MBBS1 1Deenanath Mangeshkar Hospital and Research Center, Pune, Maharashtra, India; 2Shivanand Desai Center for Digestive Disorders, Deenanath Mangeshkar Hospital and Research Center, Pune, Maharashtra, India
Introduction: Recurrent hemobilia (RHB) due to intra-biliary tumor is a known etiological factor for recurrent acute cholangitis (RAC), however less often as a cause for recurrent acute pancreatitis (RAP).
This case highlights a rare tumor – sarcomatoid gall bladder carcinoma resulting in recurrent cholangitis and pancreatitis, possibly due to recurrent hemobilia.
Case Description/Methods: 42-yr female – h/o 4 episodes RAP x 5-months, one severe – hospitalisation (elsewhere). Abdominal CT – CBD calculi, gall bladder – sludge, liver biochemistry (LFTs) – obstructive pattern. ERCP – sludge and pus drained, 7Fr. plastic biliary stent (PBS). Spontaneous distal migration of PBS subsequently. Elective cholecystectomy scheduled.
4-weeks later (our center) hospitalized – abdominal pain, fever, leucocytosis. CT Abdomen, EUS – resolving AP, portal vein thrombosis, biliary dilatation but no stones, cholangitic hepatic abscesses. Clinical response to antibiotics, hence discharged on newer oral anticoagulant.
Second hospitalization (2-weeks later) – abdominal pain, fever, leucocytosis, deteriorating LFTs. ERCP – dilated biliary tree + sludge ; balloon clearance of sludge and clots. No residual filling defect. 7Fr. PBS placed. 2 days later – melena with hemoglobin drop.
EGD and CT abdominal angiography – normal. No further bleed, discharged.
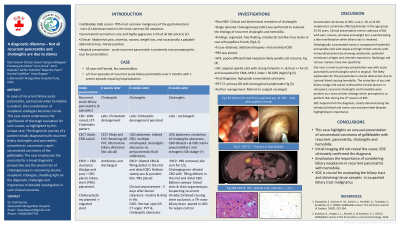
4-weeks later 3rd hospitalization for RAC. Repeat ERCP – multiple intraductal blood clots (Fig A) and pus, balloon clearance, 7Fr. nasobiliary drain for sepsis control.
After cholangitis settled, underwent single-operator cholangioscopy (SOC) – organised free-floating intraductal cast / clot-like mass lesion with papillary fronds. Balloon clearance, specimen (cast) sent for histopathology. Additional SOC guided biopsies, PBS placed.
Histopathology & IHC (Fig B & C) (cast + biopsy) – high grade sarcomatoid carcinoma. Subsequent PET CT – primary lesion in gall bladder body. Patient advised oncosurgery consult.
Discussion: This case illustrates an unusual presentation of a rare tumor – gall bladder sarcomatoid carcinoma presenting with RAP, RAC and RHB. Initial imaging failed to identify the primary etiology and finally SOC confirmed the diagnosis. The case highlights that all recurrent biliary AP may not be due to stone disease, and RHB should raise suspicion of a biliary neoplastic cause.
Figure: Fig A : Repeat ERCP balloon swipe showed large blood clots Fig B : 40x H & E stain Showing poorly differentiated neoplasm suggestive of spindle cell sarcoma. Fig C : Occasional EMA positivity on IHC
Note: The table for this abstract can be viewed in the ePoster Gallery section of the ACG 2024 ePoster Site or in The American Journal of Gastroenterology's abstract supplement issue, both of which will be available starting October 27, 2024.
Disclosures:
Yash Kanani indicated no relevant financial relationships.
Chetan Oswal indicated no relevant financial relationships.
Sanjana Bhagwat indicated no relevant financial relationships.
Chaitaniya Kumbhar indicated no relevant financial relationships.
Arun Arora Pagadapelli indicated no relevant financial relationships.
Amit Daphale indicated no relevant financial relationships.
Sachin Palnitkar indicated no relevant financial relationships.
Rajendra Pujari indicated no relevant financial relationships.
Harshal Gadhikar indicated no relevant financial relationships.
Amol Bapaye indicated no relevant financial relationships.
Yash Kanani, MBBS, MD1, Chetan Oswal, Mbbs, MD1, Sanjana Bhagwat, MBBS, MD1, Chaitaniya Kumbhar, MBBS, MD1, Arun Arora Pagadapelli, MBBS1, Amit Daphale, MBBS2, Sachin Palnitkar, MBBS, MD, DM1, Rajendra Pujari, MBBS, MD, MRCP1, Harshal Gadhikar, MBBS, MD, DM1, Amol Bapaye, MBBS1. P1879 - A Diagnostic Dilemma – Not All Recurrent Pancreatitis and Cholangitis Are Due to Stones!, ACG 2024 Annual Scientific Meeting Abstracts. Philadelphia, PA: American College of Gastroenterology.


 photo")
